
From the 1Department of Community Medicine and Rehabilitation, Umeå University, Umeå, 2Department of Research, Region Norrbotten, Luleå and 3Department of Health Sciences, Division of Occupational Therapy, Luleå University of Technology, Luleå, Sweden
Objective: To evaluate patient-reported outcome measures in 2 different multimodal pain rehabilitation programmes and to determine whether outcomes are related to sex or age at 1-year follow-up.
Design: Longitudinal retrospective study.
Subjects: Patients who had participated in 1 of 2 multimodal pain rehabilitation programmes at 2 rehabilitation centres. A total of 356 women and 83 men, divided into 3 age groups.
Methods: Data from the Swedish Quality Registry for Pain Rehabilitation regarding activity and physical functions, pain intensity, health status and emotional functions analysed with descriptive statistics.
Results: Significant improvements in activity and physical functions, pain intensity and emotional func-tions were found in both multimodal pain rehabilitation programmes. Women improved more than men. The older group improved in all emotional functions (depression, anxiety, mental component summary), while the younger group improved only in depression. The intermediate group improved in all variables except anxiety.
Conclusion: Patients improved regardless of the design of the multimodal pain rehabilitation programme. Although only small differences were found between men and women and among the 3 age groups in terms of the measured variables, these findings may have clinical relevance and indicate a need to vary the design of the interventions in multimodal rehabilitation programmes for these subgroups.
Key word: chronic pain; musculoskeletal pain; rehabilitation; sex; age.
Accepted Apr 11, 2018; Epub ahead of print Jun 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Linda Spinord, Department of Research and Development, Region Norrbotten and Department of Community Medicine and Rehabilitation, Umeå University, Rehabilitation Medicin, SE-90187 Umeå, Sweden. E-mail: linda.spinord@norrbotten.se
Multimodal rehabilitation has been shown to be an effective form of rehabilitation for people with chronic pain. This study investigated 2 different multimodal pain rehabilitation programmes in northern Sweden and evaluated patient-reported outcomes to determine whether outcomes were related to sex or age at 1-year follow-up. In both programmes, women improved more than men and the improvements in the age groups differed between the programmes. These findings may indicate a need to vary the design of the interventions in rehabilitation programmes for these subgroups.
It is well-known that chronic pain can have negative effects on a number of aspects of daily life, such as participation in society during both leisure and working time, as well as total life satisfaction (1, 2). In addition, chronic pain may have psychological consequences, such as anxiety and depression (3). Since chronic pain is a complex condition with multifaceted origins and consequences (4, 5), a biopsychosocial approach is important for treatment and rehabilitation. To include the different aspects of a patient’s life, multimodal rehabilitation (MMR) is a team-based cognitive-behavioural therapy programme, which involves interventions that consider different aspects of chronic pain (6). Common components of MMR are education, coping skills and physical activity/training. Although it has been shown that MMR programmes are more effective than unimodal treatment (7–9), there are no clear published guidelines regarding how MMR should be designed in terms of programme length and which combinations of interventions are most effective. Despite this uncertainty about optimal MMR, the common concept is based on the biopsychosocial model. Moreover, since studies of MMR usually lack detailed descriptions of the content of the intervention, the type of personnel who delivered the treatment, and the intensity of the programmes, these factors have been identified as knowledge gaps (9). There is also uncertainty regarding the effects of MMR on men and women, respectively, and for people of different ages.
Women are over-represented in MMR (9) since almost 80% of participants in MMR programmes in Sweden are women (10). Research has shown that women report a higher prevalence of chronic pain, more pain sites and longer duration of pain than men (11). Although it has been shown that men and women benefit unequally from MMR regarding pain parameters, emotional functions and activity in daily life (12), there is still a lack of knowledge regarding the results for women and men, respectively.
Most MMR programmes include adult patients of working age from 18 to 65 years. This is a wide age range and the mean age of the patients in MMR programmes in Sweden is 43 years (10). In previous research, age has commonly been used as an outcome predictor, and younger age has been shown to predict a positive outcome in terms of health-related quality of life (HRQoL) (13, 14) and physical functions (15) after MMR. Few studies (13, 16) have focused on the results in separate groups of younger and older adults, and therefore there is limited knowledge about the effects of MMR in different age groups.
In northern Sweden, which has geographically dispersed and sparsely populated areas, patients may need to travel long distances to rehabilitation clinics and specialized healthcare. Those circumstances may lead to different designs and settings of the MMR programmes in these areas. Since there is a lack of knowledge in the literature regarding how differences in MMR, such as the content, intensity and length of the programmes, may affect outcomes, we conducted a study based on 1-year follow-up data from the Swedish Quality Registry for Pain Rehabilitation (SQRP) for 2 different MMR programmes.
The aims of this study were: (i) to evaluate patient-reported outcome measures (PROMs) in 2 different MMR programmes; and (ii) to determine whether outcomes were related to sex or age.
The investigation comprised a longitudinal, retrospective study with 1-year follow-up of 2 different MMR programmes in 2 different settings and county councils in northern Sweden: the Pain Rehabilitation Clinic, Umeå University Hospital (Programme U) and the Department of Rehabilitation Medicine, Sunderby County Hospital (Programme S). The majority of the patients had been referred to the hospitals by primary healthcare services. In both programmes, the patients were assessed by multi-professional teams before their participation in MMR. In the MMR programmes, the patients created a rehabilitation plan together with the team and they were encouraged to take an active role in goal-setting. The majority of the interventions were conducted in group sessions of approximately 6 h/day, based on cognitive-behavioural principles (17). The sessions with a physiotherapist included guided exercise, body awareness and relaxation. In the occupational therapist sessions, the focus was on ergonomic/occupational performance habits, experience-based learning, pacing with a focus on doing, and balancing rest and activities. The psychologist sessions included stress management, coping strategies, acceptance and psychological reactions to chronic pain. The lectures by a physician in rehabilitation medicine (Programme U) focused on information about bodily reactions to chronic pain and medication. The nurse/health coach (Programme S) focused on medication, relaxation, diet and nutrition. The social worker focused on information regarding society. When needed, the patients could receive individually tailored sessions with different members of the team. The general goals for the programmes were to reduce pain intensity, improve activity and life satisfaction, and improve the patients’ coping strategies to allow them to achieve their individual goals.
At the end of the programme, contact was established with external collaborating partners, such as the patient’s general practitioner, the Swedish Social Insurance Agency and the workplace.
The main differences between the U and S programmes were the length of the programmes, the geographical location and the professionals in the team. In Programme U, both the assessment and the MMR were conducted by the same team of professionals in the same geographical location, the University Hospital. In Programme S, there were different people in the assessment team and in the MMR team: a nurse but no physician participated in the MMR team. The assessment was performed at the hospital, but the MMR programme was conducted in another clinical setting, 30 km from the hospital. In addition, most of the Programme U patients lived at home during the MMR period, while for Programme S, all patients stayed at a patient hotel during the MMR (Table I).
Table I. Differences between the multimodal rehabilitation (MMR) programmes
All the patients who participated in MMR and completed the questionnaires in the SQRP from 2011 to 2015 were included (Fig. 1). Inclusion criteria for participating in MMR according to the SQRP were disabling non-malignant musculoskeletal chronic pain for >3 months and age between 18 and 65 years. Exclusion criteria were: (i) ongoing major somatic (i.e. heart diseases, cancer, etc.), or psychiatric (schizophrenia, severe depression, etc.) disease; and (ii) substance abuse (i.e. alcohol, narcotics, or addictive medication). The participants were divided into 3 age groups: a younger group (18–30 years), an intermediate group (31–45 years) and an older group (46–65 years).
Fig. 1. Flow of patients at start, after and at 1-year follow-up of multimodal rehabilitation (MMR), n (%).
This study initially included 439 patients with chronic pain, both local pain (neck pain, back pain) and general pain allocated to MMR Programme U (n = 220, 177 women and 43 men) and MMR Programme S (n = 219, 179 women and 40 men). At 1-year follow-up after MMR, the attendance rates were 62% for Programme U and 71% for Programme S (Fig. 1).
The SQRP is a national database for patients age 18–65 years with complex chronic non-malignant musculoskeletal pain (<3 months). The registry started in 1998. It is based on questionnaires and is recognized by the Swedish Association of Local Authorities and Regions (SALAR). The SQRP aims to monitor outcomes of a rehabilitation process in order to facilitate comparisons of specialized pain rehabilitation clinics. The registry evaluates and develops the quality of specialized pain rehabilitation clinics that treat patients with MMR. Data from the assessment of patients and self-reported data from patients participating in MMR are presented in the SQRP. The main purpose of the registry is to present results of MMR at a group level to participating clinical departments and compare the patient groups at different rehabilitation clinics and the effect of rehabilitation programmes according to Patient-Reported Outcome Measures (PROM) concerning function, activity, quality of life and participation in working life and leisure. Patients are referred mostly from primary healthcare to rehabilitation clinics. The patients participating in MMR complete questionnaires before, after and at 1-year follow-up. The units collect data in accordance with the SQPR’s written instructions. The questionnaires are either posted to patients prior to a first visit or administered on site. The 1-year follow-up is usually sent by post, including one reminder. Ninety percent of the rehabilitation clinics at a specialized level in Sweden (31 units in June 2015), reported patient data during the data collection period. The SQRP registry reported n = 2,610 patients at 1-year follow-up for patients who had completed their MMR in 2015.
The patients completed questionnaires with PROM at the start of MMR, after MMR and at the 1-year follow-up. The questionnaires were included in the SQRP. At the 1-year follow-up, the questionnaires were sent home to be returned by post in a prepaid addressed envelope. If no answer was received within 4 weeks a reminder was sent to the patient. The questionnaires included demographics and questions regarding pain duration, number of pain sites and intensity, as well as education, country of birth, work situation and sick leave. In this study, 5 instruments from the SQRP were included: Multidimensional Pain Inventory (MPI) (18), EuroQol 5D (EQ5D) (19), Hospital Anxiety and Depression Scale (HADS) (20), Numeric Pain Rating Scale (NPRS) (21), and Short Form health survey (SF-36) (22). For detailed description of the instruments, see Table II. The instruments were categorized into 5 domains: activity functions (MPI interference), physical functions (SF-36 PCS), pain intensity (MPI pain, NPRS), health (EQVAS) and emotional functions (HADS A, HADS A ≥ 11, HAD D, HAD D ≥11 and SF36 MCS), mainly according to the recommendations of the IMMPACT group (23). The results were reported in domains and the current variables in parentheses. In this study, data from the start and 1-year follow-up were used.
Table II. Instruments
Analyses according to sex and age groups were performed in 2 steps in order to analyse both groups together and separately in the 2 programmes. In step one, the 2 populations were combined and the outcomes for women, men and age groups were analysed. In step 2, the populations were split up into the 2 programmes (Programmes S and U) and analysed separately.
All statistical analyses were performed using the statistical package IBM SPSS 24.0. For all questionnaires concerning PROM, non-parametric statistics were used. Results with p-value < 0.05 (2-sided) were considered significant for all tests. For comparisons of median values, the Mann–Whitney U test and Kruskal–Wallis test were used. The changes between baseline and 1-year follow-up were tested with Wilcoxon’s signed-rank test. The data are presented as median and interquartile range and as counts and percentages for categorical variables. In MPI interference, a decrease ≥ 0.6 and a decrease in NRPS ≥ 30% are defined as Minimal Clinically Important Differences (MCID) (24).
This study was conducted in accordance with the Declaration of Helsinki and was approved by the regional Ethical Review Board of Umeå University (reference number: 2015/240-31).
No significant differences in terms of sex, education, sick leave, pain duration, activity, physical functions and health were found between participants and dropouts. In both programmes, the dropouts had a lower mean age (p = 0.012; < 0.0001). In Programme S, the dropouts had lower pain intensity (NPRS p = 0.044) and lower emotional functions (SF-36MCS p = 0.008) compared with participants.
The participants included in Programme U were significantly younger, fewer were on sick leave, they reported fewer days with chronic pain, and were more likely to be employed compared with those included in Programme S (Table III). There were no significant differences in the PROM between the participants in the 2 programmes.
Table III. Demographic data, pain characteristics and patient-reported outcome measures at start of the 2 programmes
No significant differences between men and women in terms of age, country of birth, livelihood or PROM results were found. Women reported a significantly higher mean number of pain sites (women n=16, men n = 12, p < 0.0001), percentage with university degree (women 36%, men 18%, p = 0.030), and amount of sick leave (women 65%, men 40%, p = 0.018) compared with men at the start of the MMR programmes.
In both programmes, women reported a significantly higher mean number of pain sites (U: women n = 15, men n = 12, p = 0.009. S: women n = 16, men n = 12, p = 0.001). Despite that, more men than women reported chronic pain for >2 years.
Comparison of age groups revealed significant differences in days with chronic pain (p = 0.037) and emotional functions (HADS A, SF-36 MCS). 45% of the youngest group reported ≥ 11 in HADS A, while only 20% of the older group reported ≥ 11 in HADS A (Table IV).
Within the age groups, the older adults (46–65 years) reported better mental health compared with the other 2 age groups (p ≤ 0.028 SF-36 MCS, HADS A). In addition, the young adult group reported better physical function than the oldest age group (p = 0.24 SF-36 PCS).
In the separate analysis of the programmes, the young adults were more likely to be unemployed or students compared with the other age groups in programme U. The older adults reported better mental health (p ≤ 0.048 HADS A) and worse physical functions (p = 0.049 SF-36 PCS) compared with the other 2 age groups.
In Programme S, fewer of the young adult participants were employed, and they reported higher scores for anxiety (p ≤ 0.04 HADS A) compared with the other 2 age groups.
Table IV. Patient-reported outcomes measures at start in age groups
At 1-year follow-up, patients in both MMR programmes had improved significantly regarding activity in daily life (MPI interference) pain intensity (NPRS) and emotional functions (HADS A, HADS A ≥ 11, HADS D, SF-36 MCS). Participants in Programme U had improved significantly regarding physical functions (SF-36 PCS) and health (EQ5D VAS). According to MPI interference, MCID were achieved for 46.7% in Programme U and for 26.5% in Programme S (Table V).
Table V. Changes from start to 1-year follow-up in the 2 multimodal rehabilitation (MMR) programmes
Significant improvements were found among men and women regarding activity in daily life (MPI interference), pain intensity (NPRS), health (EQ5D-VAS) and emotional functions (HADS A ≥ 11, HADS D, HAD D ≥ 11). Women also reported significant improvements in physical functions (SF-36 PCS), pain intensity (MPI pain severity) and emotional functions (HADS A, SF-36 MCS) (Table VI).
Table VI. Changes from start to follow-up in women and men separately
For Programme U, Table VII shows that significant improvements were found among men and women regarding activity and physical functions (MPI interference, SF-36 PCS), and pain intensity (NPRS, MPI Pain Severity). Women showed significant improvements in health (EQ5D-VAS) and emotional functions (HADS A, HADS D, SF-36 MCS). According to MPI interference, MCID were achieved for 56% of the men and 44.7% of the women and according to NRPS, MCID were shown for 26% of the men and 24.6% of the women.
Table VII. Number of improved variables at 1-year follow-up in women and men in the 2 different multimodal rehabilitation (MMR) programmes
In Programme S, women showed significant improvements in activity in daily life (MPI interference), pain intensity (NPRS, MPI pain severity) and emotional functions (HADS A, HADS D, SF-36 MCS). Men reported significant improvements in pain intensity (NPRS) and emotional functions (HADS D, HADS D ≥ 11) (Table VII). According to MPI interference, MCID were shown for 11.5% of the men and 29.5% of the women. In NRPS, MCID were shown for 26.9% of the men and 29.5% of the women.
All age groups showed significant improvement in activity in daily life (MPI interference), pain intensity (NPRS, MPI pain severity), and emotional functions (HADS D). The intermediate group improved in most variables. The youngest age group improved most according to MCID in NPRS (Table VIII).
When the 2 programmes were analysed separately, Programme U showed significant improvement in all 3 age groups for activity and physical function (MPI interference, SF-36 PCS) and pain intensity (NPRS). The older adults showed most improvements in pain intensity (MPI pain severity), anxiety (HADS A) and depression (HADS D). The intermediate age group showed significant improvements in pain intensity (MPI pain severity) and health (EQ5D VAS) (Table IX). In MPI interference, MCID were achieved for 44% of the youngest group, 43.6% of the intermediate group and 50.9% of the oldest group. According to NRPS, MCID were achieved for 32% of the youngest group, 20% of the intermediate group and 26.3% of the oldest group.
In Programme S, all the age groups showed significant improvements in pain intensity (NPRS, MPI pain severity) and depression (HADS D, HADS D ≥11). The younger and older adults reported significant improvements in emotional functions (SF-36 MCS, HADS A). The younger adults (18–30 years) reported improvements in health (EQ5D VAS). The older adults (46–65 years) reported significant improvements in activity in daily life (MPI interference) and emotional functions (HADS A ≥ 11 (Table IX). According to MPI interference, MCID were achieved for 25% of the youngest group, 23.1% of the intermediate group and 28.6% of the oldest group. In NRPS, MCID were achieved for 50% of the youngest group, 26.9% of the intermediate group and 27.5% of the oldest group.
Table IX. Number of improved variables at 1-year follow-up in age groups in the 2 different multimodal rehabilitation (MMR) programmes
In this study, the PROM in participants with chronic pain from 2 differently designed MMR programmes in northern Sweden were studied at the start of MMR and at 1-year follow-up. The results indicate improvements in emotional functions, pain intensity, activity in daily life and physical functions at 1-year follow-up for participants who had participated in 1 of the 2 programmes. Women improved more than men and there were differences between the age groups regarding the outcomes measures related to baseline.
The rehabilitation programme interventions for chronic pain are unique in the sense that the participants themselves play a crucial role in the rehabilitation process and participation in the MMR interventions as an active team member. The findings of improvements in emotional function, pain intensity and activity in daily life in this study confirm the generally positive results found in previous studies of MMR (9, 26–29).
A higher percentage of participants in Programme U reached the MCID on the MPI interference scale than the participants in Programme U at 1-year follow-up related to baseline. A possible explanation could be that the participants in Programme U were younger, fewer were on sick leave and they were more likely to be employed compared with the participants in Programme S at the start of the programme. Another aspect of the MCID in MPI interference could be the differences between the programmes.
This study was an attempt to address the knowledge gap regarding different MMR programmes (content of the interventions, who delivered the treatment, and the intensity of the MMR) in relation to the long-term outcomes. Although there were some differences between the 2 MMR programmes regarding the length of the programmes and the different professionals who took part, both programmes seem to have effectively addressed the aspects of chronic pain.
More women than men participated in this study. It is well-known that women have a higher prevalence of chronic pain than men (11). This could explain the higher proportion of women included and participating in MMR (14, 30). It is interesting that in both programmes, the men reported longer pain duration before participating in MMR compared with the women. This could be because men are more likely to receive recommendations for unimodal methods, such as physiotherapy (31), and if these treatments are insufficient, they may then be referred to MMR at a later stage. Moreover, healthcare professionals’ attitudes and preconceptions regarding which participants are appropriate for MMR might also result in men being referred later. Another possible sex difference is the observation made by Ahlsen et al. (32), that the physicians in primary care hesitated to diagnose men with disorders such as chronic pain or fibromyalgia because they could be perceived as being unmanly.
In this study, there were no significant differences between the men’s and women’s PROMs prior to participation in MMR. However, differences between women and men were found in terms of outcome measures following MMR, related to baseline. In addition, in both programmes women improved on more variables than did men. This confirms findings from previous research (12, 33) and may be explained by the participants’ expectations of MMR. Research has found that women are able to find strategies that help them to cope with their situation, while men are often more focused on the biomedical approach (34). In addition, because most patients who are offered and undergo MMR are women, programmes may be better adapted to women’s needs. In the present study, we found that, despite the different designs of the MMR programmes, women perceived greater effects than men. Hence, one suggestion is to adapt the content to better support individual prerequisites and expectations from MMR.
The participants were divided into 3 age groups (younger adults 18–30 years, intermediate age 31–45 years, older adults 46–65 years). At the start of the MMR programme, a majority of the assessed variables were similar for the 3 age groups in both programmes. Still, significant differences were found between the age groups in each programme in terms of anxiety. Overall, the younger adults reported higher scores in anxiety (HAD A) than the other age groups. These results are in line with previous research in which anxiety and depression are reported to be more common among younger patients (35). This could explain the higher proportion of self-reported anxiety in our study.
Our results show that all age groups improve in activity in daily life, pain intensity and depression, but on the basis of our findings, it seems that participants in different age groups may have different needs when participating in MMR. In our study, the intermediate group had better results in Programme U, related to baseline. Since most participants were living at home during the MMR in Programme U, a possible explanation could be that participants in the 31–45-year age group may have children at home and it was easier to incorporate the rehabilitation into their family situation if they did not have to be away for several weeks. In a previous study by Boonstra et al. (15), patients with children ≤ 12 years were more likely to participate in outpatient treatment programmes. However, the register we used in this study, SQRP, does not include any demographic information regarding whether participants are parents.
Some previous long-term 1-year follow-up studies have shown that the pattern of full-time sickness absence decreased after MMR (35, 36). In this study, part-time sick leave decreased 1 year after MMR, while full-time sick leave did not decrease. At the end of the programmes, contacts were established with external collaborating partners, such as the workplace, the social insurance agency and the patient’s general practitioner. However, this was not mandatory. Therefore a possible explanation is that neither of the 2 MMR programmes provided specific work-directed interventions for all participants at the time of the data collection. Work-directed interventions have been viewed as being an important factor for return to work (37). However, since the data collection period, work-directed interventions have been added to both MMR programmes. In the future, it would be interesting to study the effects of these interventions on return to work.
Some limitations of the study should be noted. Reliability is an issue in every type of study. However, the data in this study were retrieved from the SQRP, and all instruments are widely used and have shown good validity. In addition, all assessments were performed using standardized procedures and well-established outcome measures. It is possible that the dropouts may have influenced the results, since the drop-out rates were relatively high. However, the 1-year follow-up rates in this study were relatively good compared with other studies that also used the SQRP (38, 39). One limitation of our study was the lack of a control group, because our data were generated in a clinical setting in ordinary healthcare. Another potential limitation was that only patients who completed the SQRP questionnaires at baseline and at follow-up were included, Intention to treat analyses were not applied. This could be an explanation for the positive outcomes of the study, as ITT analyses may reduce effect sizes. It could be argued that the changes observed represent a spontaneous improvement over time. However, it is known that once chronic pain has become established, it is unlikely to resolve itself without intervention (40).
In conclusion, the participants in either of 2 different MMR programmes in northern Sweden improved in terms of emotional function, pain intensity and activities of daily life, regardless of the design of the programme. Secondly, there were some minor differences between men and women and between the different age groups. These differences could suggest a need to vary the design of interventions in MMR programmes for specific subgroups.
The study was supported by grants from Region Norrbotten.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize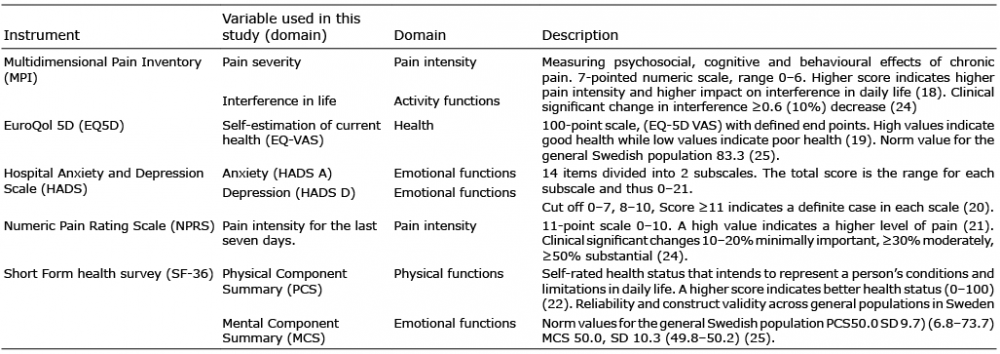 Click to show fullsize
Click to show fullsize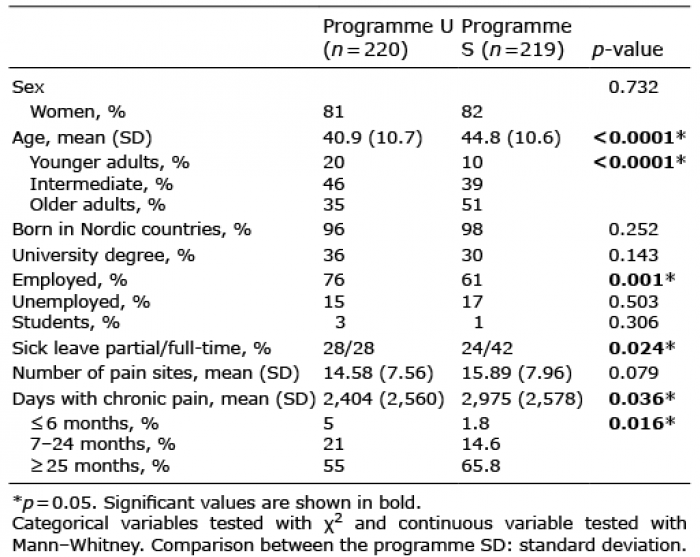 Click to show fullsize
Click to show fullsize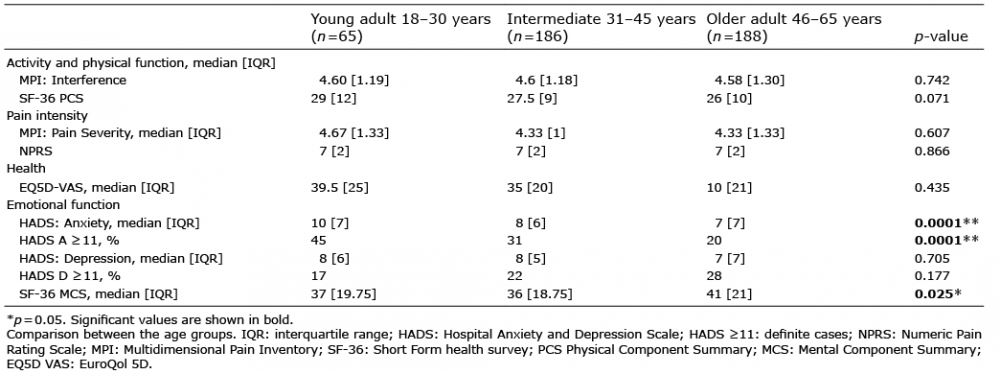 Click to show fullsize
Click to show fullsize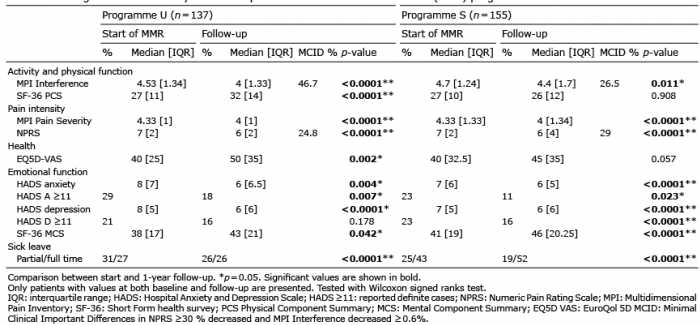 Click to show fullsize
Click to show fullsize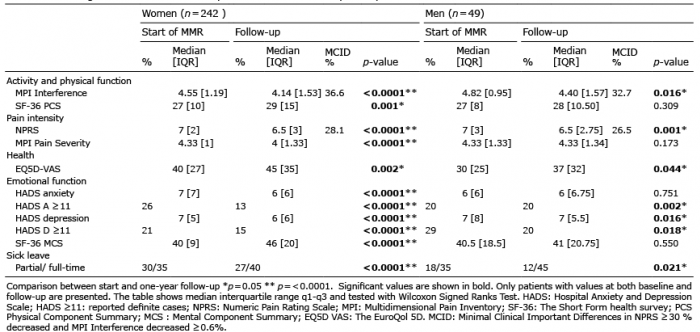 Click to show fullsize
Click to show fullsize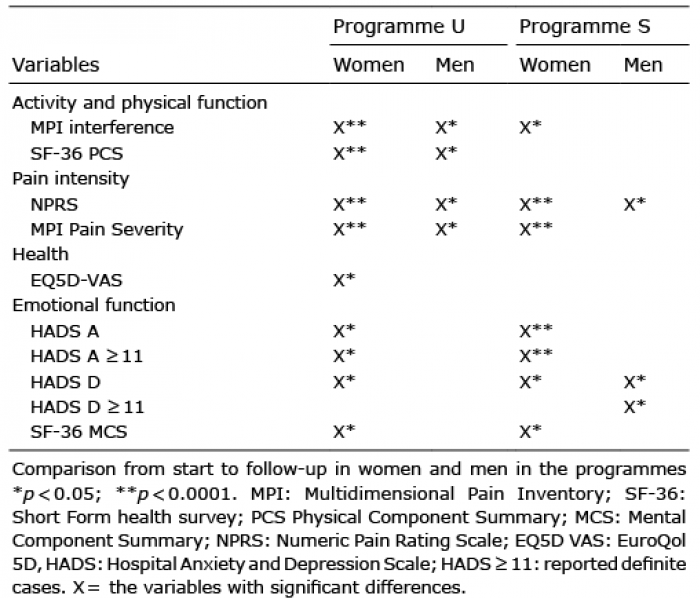 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize